94 questions match your search.
When compared with a healthy 30-year-old man, which of the following respiratory parameters is decreased in an otherwise healthy 80-year-old man?
- (A) Alveolar to arterial oxygen gradient
- (B) Lung compliance
- (C) Ratio of functional residual capacity to total lung capacity
- (D) Resting tidal volume
- (E) Ventilatory response to carbon dioxide
A sensory level of T2 is achieved after administration of spinal anesthesia. Which of the following lung volumes is LEAST likely to be affected?
- (A) Expiratory reserve volume
- (B) Inspiratory reserve volume
- (C) Inspiratory capacity
- (D) Tidal volume
- (E) Vital capacity
A 60-kg 25-year-old woman is undergoing laparoscopy in the Trendelenburg position during general anesthesia. Five minutes after peritoneal inflation, the peak airway pressure required to deliver a tidal volume of 800 ml increases from 25 cmH2O to 60 cmH2O. SpO2 decreases from 100% to 80% and systolic blood pressure increases from 110 mmHg to 140 mmHg. Which of the following is the most likely cause?
- (A) Acute tension pneumothorax
- (B) Excessively steep Trendelenburg position
- (C) Excessive ventilator tidal volume setting
- (D) Kink in the endotracheal tube
- (E) Massive carbon dioxide embolism
After tracheal extubation, a healthy 21-year-old man has a 30-second episode of laryngospasm with marked intercostal and sternal retractions, which are corrected with continuous positive airway pressure administered by mask. He now has dyspnea and tachypnea, and a roentgenogram of the chest shows diffuse bilateral interstitial edema. The most likely cause is increased
- (A) airway reactivity
- (B) intrapleural pressure
- (C) left ventricular afterload
- (D) right ventricular preload
- (E) transpulmonary vascular pressure
A 50-year-old man with an 80 pack-year history of cigarette smoking has a forced expiratory volume in one second of 1.5 L and a forced vital capacity of 3.5 L. Which of the following statements concerning intraoperative anesthetic management is true?
- (A) An I:E ratio of 1:1 will improve carbon dioxide removal more than an I:E ratio of 1:2.5
- (B) Antagonism of neuromuscular block will most likely trigger acute bronchospasm
- (C) Functional residual capacity will increase during an acute exacerbation of bronchospasm
- (D) Induction with ketamine will increase airway resistance
- (E) Nitrous oxide is contraindicated
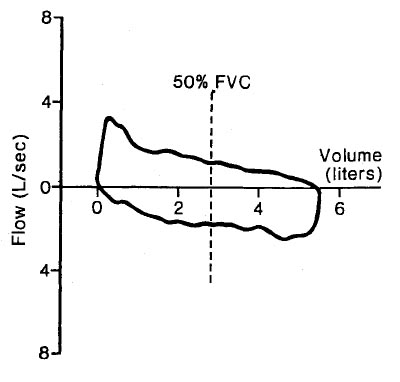
The flow-volume loop indicated by the "X" is characteristic of
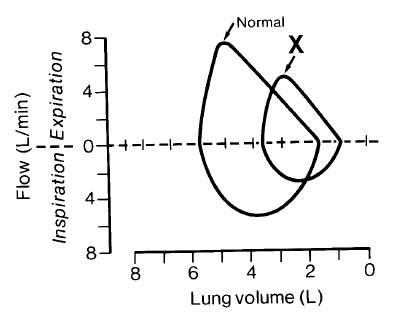
- (A) asthma
- (B) bronchiectasis
- (C) emphysema
- (D) pulmonary fibrosis
- (E) tracheal stenosis
The illustration depicts flow-volume loops for the same person at two different times in his life. Which of the following is indicated by the dotted loop?
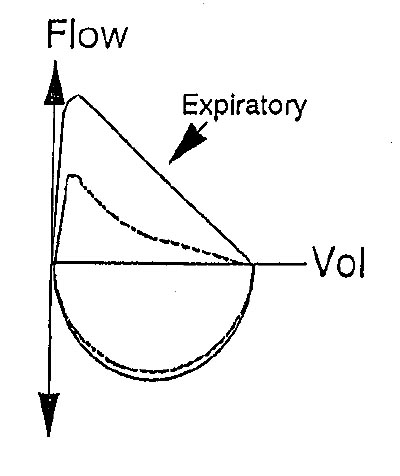
- (A) Bronchial tumor
- (B) Chronic asthmatic bronchitis
- (C) Morbid obesity
- (D) Paralysis of a vocal cord
- (E) Subglottic stenosis
Cessation of smoking on the day prior to an operation is associated with a perioperative
- (A) decrease in carbon monoxide in blood
- (B) improvement in ciliary beating in the airways
- (C) decrease in sputum volume
- (D) decrease in the need for postoperative ventilatory support
- (E) decrease in the risk of deep vein thrombosis
Which of the following is the most likely cause of a decrease in end-tidal carbon dioxide tension during general anesthesia with a constant minute ventilation?
- (A) Administration of sodium bicarbonate
- (B) Intravenous administration of hypertonic glucose solution
- (C) Decrease in cardiac output
- (D) Decrease in fresh gas flow in a Bain circuit
- (E) Malfunction of the inspiratory valve in a circle system
Static lung compliance is decreased by each of the following EXCEPT
- (A) pulmonary emphysema
- (B) congestive heart failure
- (C) adult respiratory distress syndrome
- (D) pulmonary fibrosis
- (E) inhalational anesthesia
Each of the following increases arterial to end-tidal carbon dioxide tension difference EXCEPT
- (A) addition of positive-end expiratory pressure
- (B) deliberate hypotension
- (C) endobronchial intubation
- (D) hypovolemia
- (E) pulmonary embolism
A 54-year-old man is scheduled for open reduction of a fracture sustained when he jumped from a burning building. The carboxyhemoglobin concentration is 25%. Which of the following is the most reliable indicator of adequate oxygenation during general anesthesia?
- (A) PaO2 of 300 mmHg
- (B) pH of 7.38 with a PaCO2 of 41 mmHg
- (C) Mixed venous PO2 of 45 mmHg
- (D) Oxyhemoglobin saturation of 100% measured by co-oximeter
- (E) SpO2 of 100% measured by pulse oximeter
Microatelectasis 48 hours after abdominal surgery is most consistently manifested by
- (A) decreased PaO2
- (B) ground glass infiltrate on a roentgenogram of the chest
- (C) scattered fine inspiratory rales
- (D) increased PaCO2
- (E) scattered areas of dullness to chest percussion
Each of the following is a physiologic effect of intra-aortic balloon pump therapy EXCEPT
- (A) decreased peak systolic pressure
- (B) increased cardiac output
- (C) increased coronary perfusion
- (D) increased diastolic pressure
- (E) increased total peripheral resistance
Initiation of positive pressure mechanical ventilation is LEAST likely to decrease cardiac output in patients with which of the following conditions?
- (A) Abdominal distention with decreased lung volume
- (B) Acute cardiogenic pulmonary edema
- (C) Chronic obstructive pulmonary disease
- (D) Flail chest following an automobile accident
- (E) 20% Right pneumothorax
During apneic oxygenation (FiO2 1.0) through a rigid bronchoscope
- (A) duration of the procedure is limited by the increase in PaCO2
- (B) functional residual capacity decreases 5%/min
- (C) PaO2 remains unchanged for the first 5 minutes
- (D) PaCO2 increases 2 to 6 mmHg/min for 15 minutes and then reaches a plateau
- (E) PaO2 and PaCO2 equilibrate with mixed venous gases at the same rate
The flow-volume loop shown is most likely from a patient with which of the following?
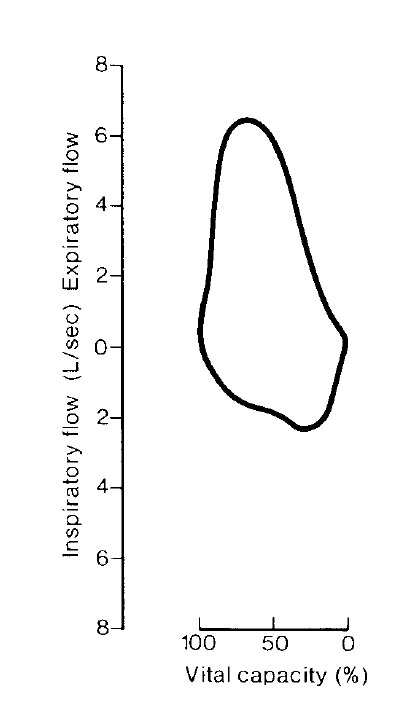
- (A) Bilateral vocal cord paralysis
- (B) Chronic bronchitis
- (C) Tracheal stenosis six months after a previous tracheostomy
- (D) Tumor of the lower trachea
- (E) Normal respiratory status
Postoperatively, a patient is being mechanically ventilated by a constant-flow, pressure-cycled ventilator with the following initial settings: inspiratory/expiratory (I/E) ratio of 1:2, peak inspiratory pressure (PIP) of 25 cmH2O, and rate of 10/min. One hour later, the I/E ratio is 1:4. Which of the following would ensure that the minute ventilation is the same as that initially set?
- (A) Inflate the endotracheal tube cuff to prevent leakage
- (B) Double the respiratory rate
- (C) Decrease the expiratory pause until the I/E ratio is 1.0
- (D) Increase the PIP until the I/E ratio is 1:2
- (E) Increase the PIP to 50 cmH20
A 30-kg patient with asthma is receiving general anesthesia and being mechanically ventilated with a measured tidal volume of 300 mL. Increasing the fresh gas flow from 3 L/min to 9 L/min without changing the ventilatory rate or I:E ratio will result in
- (A) decreased physiologic dead space
- (B) increased delivered tidal volume
- (C) increased end-expired carbon dioxide
- (D) unchanged delivered minute volume
- (E) unchanged peak inspiratory pressure
Which of the following is the greatest disadvantage of pressure-cycled ventilation?
- (A) Increased I:E ratio
- (B) Increased mechanical dead space
- (C) Increased risk for barotrauma
- (D) Variable respiratory rates
- (E) Variable tidal volumes
A combined epidural and general anesthetic is used for aortofemoral bypass surgery. Just prior to extubation, the patient received morphine 5 mg through the epidural catheter. Eleven hours later, he is unresponsive while breathing 40% oxygen from a face mask. Respiratory rate is 6/min and SpO2 is 92%. Arterial blood gas analysis shows PaO2 80 mmHg, PaCO2 84 mmHg, and pH 7.16. Which of the following statements concerning this patient is true?
- (A) Hypercarbia is contributing to the decreased level of consciousness
- (B) Naloxone is ineffective for reversing the respiratory depression
- (C) The oxygen saturation is higher than expected because of the pH
- (D) The risk for respiratory depression would have been lower with subarachnoid administration of 0.5 mg morphine
- (E) Residual local anesthetic is contributing to the respiratory depression
An anesthetized, paralyzed patient is placed in the lateral position and mechanically ventilated. End-tidal PCO2 is 34 mmHg and PaCO2 is 43 mmHg. This gradient
- (A) increases during spontaneous breathing
- (B) indicates increased dead space ventilation
- (C) is caused by increased intrapulmonary shunt
- (D) reflects inhibition of hypoxic pulmonary vasoconstriction
- (E) results from increased cardiac output
The trend plot shows end-tidal gases measured during a radical neck dissection. The event occurring at A is most likely
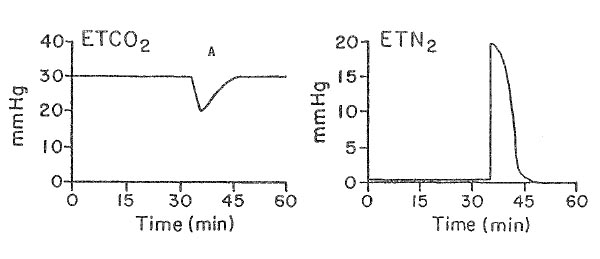
- (A) acute hypotension
- (B) endobronchial intubation
- (C) kinking of the endotracheal tube
- (D) rupture of the endotracheal cuff
- (E) venous air embolism
During application of continuous positive airway pressure, lung compliance increases because of
- (A) decreased airway resistance
- (B) decreased lung water
- (C) decreased venous return
- (D) increased intercostal muscle tone
- (E) increased resting lung volume
During general anesthesia with spontaneous ventilation, a patient has a VD/VT of 0.5. Which of the following is most likely to decrease the ratio?
- (A) Acute bronchospasm
- (B) Continuous positive airway pressure
- (C) Decreased tidal volume
- (D) Increased cardiac output
- (E) Pulmonary embolism
Which of the following statements concerning pressure support ventilation is true?
- (A) It augments gas inflow in response to spontaneous inspiration
- (B) It increases inspiratory airway pressure during controlled mandatory ventilation
- (C) It requires the use of positive end-expiratory pressure
- (D) It functions independently of airway resistance/lung compliance
- (E) It correlates linearly with spontaneously achieved tidal volume
Which of the following changes is most likely in the patient whose pulmonary pathology is schematically illustrated?
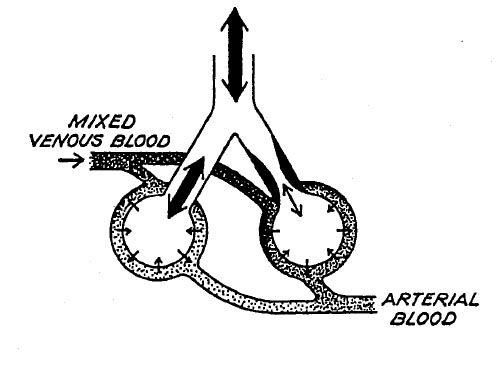
- (A) Decreased diffusing capacity
- (B) Decreased PaO2
- (C) Decreased pH
- (D) Increased PaCO2
- (E) Increased Vd/Vt
One hour after an open cholecystectomy, a 42-year-old patient is hemodynamically stable and breathing spontaneously (rate 10/min and regular) at an FiO2 of 0.4. Fentanyl, isoflurane, nitrous oxide, and pancuronium were used during the procedure. Analysis of arterial blood gases (pH, pCO2, pO2) is most likely to show:
- (A) 7.18 40 100
- (B) 7.18 60 140
- (C) 7.28 50 85
- (D) 7.40 26 220
- (E) 7.40 40 40
If minute ventilation remains constant, which of the following changes in PetCO2 and PaCO2 will result from a decrease in cardiac output? (PetCO2, PaCO2)
- (A) Decreased, Decreased
- (B) Increased, Increased
- (C) Unchanged, Unchanged
- (D) Decreased, Increased
- (E) Increased, Decreased
Blind nasotracheal intubation is contraindicated in the presence of
- (A) a basilar skull fracture
- (B) a comminuted mandibular fracture
- (C) an orbital blow-out fracture
- (D) an unstable cervical spine fracture
- (E) a zygomatic arch fracture
Which of the following statements best describes the decrease in functional residual capacity that accompanies the induction of general anesthesia?
- (A) It does not change compliance
- (B) It is greater with spontaneous ventilation than with controlled ventilation
- (C) It is independent of body position
- (D) It is not corrected by application of positive end-expiratory pressure
- (E) It occurs within the first 10 minutes of anesthesia
Addition of 20 cmH2O positive end-expiratory pressure to a patient receiving controlled mechanical ventilation decreases cardiac output and left ventricular function by
- (A) increasing right ventricular preload
- (B) increasing right ventricular afterload
- (C) increasing left ventricular preload
- (D) increasing left ventricular afterload
- (E) producing myocardial ischemia
Pulsus paradoxus is commonly seen during anesthesia in patients with each of the following conditions EXCEPT
- (A) severe asthma
- (B) right-sided heart failure
- (C) hypovolemia
- (D) atrial septal defect
- (E) obesity
After a gastric stapling procedure, a 150-kg woman is extubated and breathing spontaneously in the recovery room at a rate of 26/min and an FiO2 of 0.5. Arterial blood gas analysis shows PaO2 96 mmHg, PaCO2 44 mmHg, and pH 7.37. The parameter most closely related to her increased alveolar-arterial oxygen tension gradient is
- (A) decreased expiratory reserve volume
- (B) decreased minute volume
- (C) decreased residual volume
- (D) decreased total lung capacity
- (E) rapid respiratory rate
Which of the following pulmonary components is altered the most in a morbidly obese patient?
- (A) Total lung volume
- (B) Tidal volume
- (C) Inspiratory reserve volume
- (D) Expiratory reserve volume
- (E) Ratio of dead space to tidal volume
A patient with chronic obstructive pulmonary disease is undergoing spinal anesthesia to a T6 sensory level. The most pronounced effect on pulmonary function will be a decrease in
- (A) minute ventilation
- (B) peak expiratory flow
- (c) physiologic dead space
- (D) tidal volume
- (E) vital capacity
A patient receiving mechanical ventilation with oxygen 60% postoperatively has a PaO2 of 160 mmHg and a PaCO2 of 38 mmHg. One hour later, with mechanical ventilation unchanged, the PaO2 is 150 mmHg and PaCO2 is 48 mmHg. The most likely cause of these changes is
- (A) metabolic acidosis
- (B) pulmonary embolism
- (C) increased body temperature
- (D) interstitial pulmonary edema
- (E) aspiration pneumonia
During rapid-sequence induction prior to an emergency surgical procedure, a 20-year-old patient vomits gastric contents containing particulate matter. An endotracheal tube is easily inserted and ventilation with pure oxygen is initiated. Despite the presence of bilateral breath sounds, SpO2 is 90%. Which of the following is the most appropriate next step?
- (A) Administration of broad-spectrum antibiotics
- (B) Intravenous administration of high-dose methylprednisolone
- (C) Bronchial lavage with normal saline solution
- (D) Bronchoscopy to remove particulate matter
- (E) Cancellation of the surgical procedure
This flow-volume loop from a 57-year-old man is most consistent with which of the following conditions?
- (A) Bronchospasm
- (B) Decreased vital capacity
- (C) Myasthenia gravis
- (D) Narrowing of the upper airway
- (E) Pneumothorax
An obese, 70-year-old woman with a long history of tobacco abuse is awake and semirecumbent after uneventful anesthesia with isoflurane for a ventral hernia repair. During the first hour in the recovery room while breathing 50% oxygen by face mask, her arterial oxygen saturation decreases to 90% while other vital signs remain satisfactory. Which of the following is most likely to be effective in the management of this situation?
- (A) Intravenous doxapram
- (B) Racemic epinephrine by inhalation
- (C) Continuous positive airway pressure by mask
- (D) Reintubation of the trachea
- (E) Coughing
A healthy, spontaneously breathing, supine, anesthetized patient has a PaCO2 to PetCO2 difference of 3 mmHg. Following institution of mechanical ventilation the value increases to 12 mmHg. The most likely cause of this change is
- (A) cephalad displacement of the diaphragm
- (B) decreased production of carbon dioxide
- (C) increased cardiac output
- (D) increased shunting of blood through dependent lung zones
- (E) increased ventilation of nondependent lung zones
A previously healthy 28-year-old man is admitted to the emergency department with a probable opioid overdose. Arterial blood gas values are: PaO2 49 mmHg, PaCO2 76 mmHg, and pH 7.12 while breathing room air. Which of the following statements is true?
- (A) Aspiration of gastric contents must have occurred
- (B) Hypoventilation alone can explain the acidosis and hypoxemia
- (C) The hypoxemia is probably due to noncardiogenic pulmonary edema
- (D) Naloxone should be administered only if the patient is normothermic
- (E) Pure oxygen is contraindicated
Which of the following is the most likely cause of the increased incidence of right ventricular failure in patients with morbid obesity?
- (A) Chronic hypoxia
- (B) Chronic silent pulmonary aspiration
- (C) Chronic silent subendocardial ischemia
- (D) Decreased vital capacity
- (E) Increased pulmonary blood flow
A patient sustains cardiac arrest while being mechanically ventilated. Which of the following is the most likely effect on PetCO2?
- (A) Gradual increase with the duration of asystole
- (B) Maintenance of the prearrest value
- (C) Abrupt decrease below the prearrest value
- (D) Decrease when thoracic compression is started
- (E) Gradual decrease independent of the ventilator cycle
An apneic adult is receiving an oxygen flow of 4 L/min through a rigid bronchoscope. After five minutes of apnea, which of the following findings is most likely?
- (A) A decrease in cardiac output
- (B) A decrease in pulmonary vascular resistance
- (C) A decrease in SpO2 from 99% to 89%
- (D) An increase in PaCO2 of 18 mmHg
- (E) Serum bicarbonate concentration of 30 mEq/L
Compared with intermittent positive pressure ventilation (IPPV), intermittent mandatory ventilation (IMV)
- (A) better maintains cardiac output
- (B) provides less than full mechanical ventilatory support
- (C) requires a greater level of sedation
- (D) requires a higher FlO2
- (E) requires a lower inspiratory flow rate
Which of the following statements concerning relationships among alveolar pressure, volume, and surface tension is true?
- (A) Surface tension of surfactant decreases as alveolar volume decreases
- (B) Surface tensions of water and of surfactant behave similarly as volume decreases
- (C) Changes in alveolar surface tension with volume are the same during expansion as during contraction
- (D) Pressure in the alveolus is inversely related to surface tension
- (E) Pressure in the alveolus is directly related to alveolar radius
The carbon dioxide/ventilation response curve
- (A) is primarily a measure of the integrity of the peripheral chemoreceptors
- (B) shows parallel displacement to the left in the presence of opioids
- (C) is linear between a PaCO2 of 20 and 120 mmHg
- (D) shows progressive changes in slope with increased doses of halogenated anesthetics
- (E) is unaffected by a decrease in PaO2 to 60 mmHg
In a patient with 20% pulmonary shunt and a PaO2 of 60 mmHg, cardiac output suddenly decreases from 5 L/min to 3 L/min. Oxygen consumption is unchanged. As a result, the PaO2 will
- (A) increase slightly because of decreased shunt blood flow
- (B) decrease slightly because of decreased mixed venous PO2
- (C) increase because of decreased affinity of hemoglobin for oxygen
- (D) decrease because of an increased dead space to tidal volume ratio
- (E) increase because of increased pulmonary oxygen uptake per milliliter of blood
During anesthesia, the ventilation/perfusion ratios change
- (A) to preferential ventilation of the dependent portion
- (B) due to cephalad shift of the diaphragm
- (C) by insignificant amounts from that in the awake state
- (D) to preferential perfusion of the superior portion
- (E) from changes in pulmonary compliance
Carbon monoxide poisoning with a carboxyhemoglobin concentration of 20% is characterized by each of the following EXCEPT
- (A) decreased oxygen-carrying capacity of hemoglobin
- (B) decreased PaO2
- (C) shift of the oxyhemoglobin dissociation curve to the left
- (D) normal minute volume of ventilation
- (E) headache and nausea
A 64-year-old, 87-kg woman in good general health is undergoing a right knee arthroplasty while in the supine position with general anesthesia consisting of enflurane 2% and nitrous oxide 50% in oxygen. She is breathing spontaneously through a 7-mm endotracheal tube. During the first 30 minutes of the procedure, the arterial oxygen saturation measured by pulse oximetry decreases from 98% to 92%. The most likely cause of the desaturation is
- (A) decreased functional residual capacity
- (B) diffusion hypoxia
- (C) hypercarbia
- (D) increased airway resistance produced by the endotracheal tube
- (E) inhibition of hypoxic pulmonary vasoconstriction
If minute ventilation is held constant, which of the following is LEAST likely to alter PaCO2?
- (A) General anesthesia
- (B) Hypothermia
- (C) Increased dead space
- (D) Increased pulmonary shunt
- (E) Induced hypotension
In a patient with hypovolemic shock, which of the following factors is the best measure of the overall balance between oxygen supply and demand?
- (A) Arterial oxygen content
- (B) PetO2
- (C) Mixed venous oxygen saturation
- (D) PaO2
- (E) Transcutaneous oxygen tension
Syringe A contains 100 ml of normal blood with a PO2 of 2 mmHg, and syringe B contains 100 ml of normal blood with a PO2 of 98 mmHg. The contents of the two syringes are mixed anaerobicaily to equilibrium. The PO2 of the resultant mixture Is
- (A) 27 mmHg
- (B) 50 mmHg
- (C) 63 mmHg
- (D) 96 mmHg
- (E) 100 mmHg
A 65-kg 70-year-old man in the PACU is breathing spontaneously at 20/min through an endotracheal tube connected to a T-piece with a fresh gas flow of 5 L/min. He has a tidal volume of 350 mL and an FiO2 of 0.5. SpO2 decreases from 98% to 84% over one hour, then improves to 92% with an FiO2 of 1.0. Which of the following is the most likely cause of the hypoxemia?
- (A) Decreased functional residual capacity
- (B) Increased dead space ventilation
- (C) Inhibition of hypoxic pulmonary vasoconstriction
- (D) Room air admixture during inspiration
- (E) Shivering
Positive end-expiratory pressure is effective for treatment of hypoxia resulting from each of the following EXCEPT
- (A) cardiogenic pulmonary edema
- (B) intraoperative Trendelenburg position
- (C) lateral position during total hip replacement
- (D) lung contusion
- (E) status asthmaticus
The graphs shown illustrate various respiratory patterns in a patient who is breathing spontaneously with continuous positive airway pressure. Which of the following patterns is associated with the LEAST work of breathing?
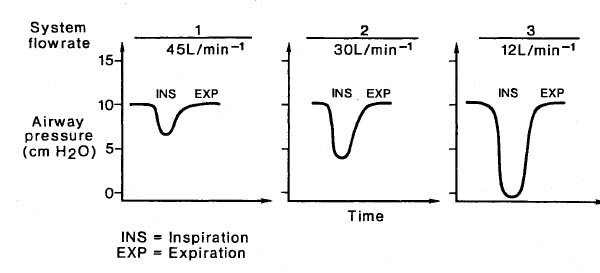
- (A) 1
- (B) 2
- (C) 3
- (D) All patterns are associated with equal work
- (E) There is not enough information to answer the question
A 70-kg, 22-year-old man who is unconscious after a closed head injury is to undergo emergency splenectomy. He is anesthetized with thiopental, given pancuronium for paralysis, and started on nitrous oxide and oxygen 50% each with controlled ventilation (tidal volume 700 ml, rate 10/min). Pulse is 70 bpm, blood pressure is 160/100 mmHg, PaO2 is 65 mmHg, PaC02 is 45 mmHg, and pH is 7.30. In adjusting the ventilator at this time, which of the following is most appropriate?
- (A) Add 10 cmH2O positive end-expiratory pressure (PEEP), increase respiratory rate to 14/min
- (B) Add sufficient PEEP to increase PaO2 to 80 mmHg
- (C) Add 10 cmH2O PEEP, increase FlO2 to 1.0
- (D) Increase tidal volume to 1000 ml, increase FiO2 to 1.0
- (E) Increase tidal volume to 1200 ml, decrease respiratory rate to 8/min
If minute ventilation remains constant, a decrease in end-expiratory carbon dioxide concentration will occur with
- (A) a decrease in physiologic dead space
- (B) a decrease in cardiac output
- (C) a decrease in physiologic shunt fraction
- (D) the development of metabolic alkalosis
- (E) an increase in body temperature
Which of the following is the most appropriate initial management of a patient with hypotension secondary to sepsis?
- (A) Calcium chloride
- (B) Corticosteroids
- (C) Crystalloid infusion
- (D) Dopamine
- (E) Fresh frozen plasma
The hemodynamic changes shown would most likely result from infusion of
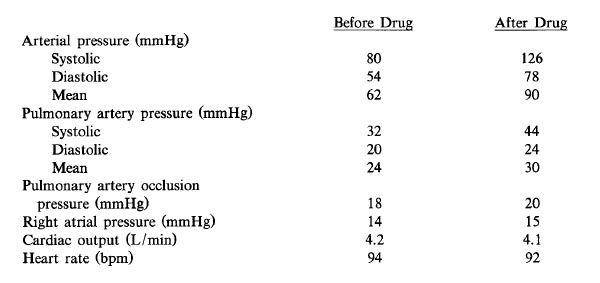
- (A) dopamine
- (B) epinepherine
- (C) dobutamine
- (D) norepinepherine
- (E) isoproterenol
Which of the following results in decreased mixed venous oxygen saturation?
- (A) Cardiogenic shock
- (B) Decreased metabolic rate
- (C) Increased cardiac output
- (D) Left-to-right intracardiac shunt
- (E) Pulmonary vasodilation
The primary purpose of denitrogenation prior to anesthetic induction is to
- (A) blunt hypoxic pulmonary vasoconstriction
- (B) improve ventilation and perfusion matching
- (C) increase contribution of second gas effect to rate of induction
- (D) increase oxygen reserve in the functional residual capacity
- (E) maximize arterial oxygen content
A 30-year-old woman is undergoing laparoscopic tubal ligation. Thirty minutes after induction of general anesthesia, arterial oxygen saturation has decreased to 89%. Arterial blood gases at an FiO2 of 1.0 are PaO2 63 mmHg and PaCO2 40 mmHg; PetCO2 is 32 mmHg. Which of the following is the most likely cause?
- (A) Carbon dioxide embolus
- (B) Endobronchial intubation
- (C) Hypoventilation
- (D) Inadvertent application of high levels of positive end-expiratory pressure
- (E) Leak in the capnography sampling catheter
Which of the following spirometric tests is most likely to be accurate in a patient with severe pain?
- (A) Forced expiratory volume in one second
- (B) Peak expiratory flow rate
- (C) Maximum midexpiratory flow
- (D) Maximum breathing capacity
- (E) Negative inspiratory pressure
Four hours after open cholecystectomy, a patient who is breathing spontaneously has an SpO2 of 93% in the supine position and an SpO2 of 98% when placed in the head-up position. The most likely cause of this change is an increase in which of the following?
- (A) Functional residual capacity
- (B) Minute ventilation
- (C) Pulmonary blood flow
- (D) Residual volume
- (E) Vital capacity
A 20-year-old man involved in a motor vehicle accident is brought to the operating room for irrigation and debridement of open fractures of the femur and humerus. Cyanosis, decreased breath sounds on the left, increased peak airway pressure, and hypotension are noted after intubation of the trachea. The most likely cause is
- (A) aspiration
- (B) fat embolus
- (C) intubation of the right mainstem bronchus
- (D) tension pneumothorax
- (E) unilateral bronchospasm
Measurement of which of the following provides the most reliable information about the severity of bronchospasm?
- (A) Diffusing capacity
- (B) Expiratory reserve volume
- (C) Forced expiratory volume in 1 second
- (D) Residual volume
- (E) Total lung capacity
High positive end-expiratory pressure can result in each of the following EXCEPT
- (A) decreased venous return
- (B) increased functional residual capacity
- (C) a left-to-right shift of the ventricular septum
- (D) decreased PaO2
- (E) pulmonary barotrauma
A 52-year-old woman undergoes facial surgery during general endotracheal anesthesia. The ventilator is set to deliver a tidal volume of 600 ml and a respiratory rate of 10/min at an FiO2 of 1.0. SpO2 is 100%, peak inspiratory pressure is 18 cmH2O, and PetCO2 is 40 mmHg. The surgeon flexes the patient's head so the chin touches the chest. Which of the following findings indicates that endobronchial intubation has NOT occurred?
- (A) Fluctuating capnographic waveform
- (B) Greater expiratory volume than inspiratory volume
- (C) Unchanged SpO2
- (D) Unchanged PetCO2
- (E) Unchanged peak inspiratory pressure
A computer program for hemodynamic calculations has the following input values: body surface area, arterial blood pressure, heart rate, pulmonary artery occlusion pressure, pulmonary artery pressure, and cardiac output. Each of the following values can be derived with this program EXCEPT
- (A) cardiac index
- (B) stroke volume index
- (C) systemic vascular resistance
- (D) pulmonary vascular resistance
- (E) left ventricular stroke work index
Which of the following statements concerning functional residual capacity is true?
- (A) It decreases linearly during a three-hour anesthetic
- (B) It decreases in pregnancy primarily because of a decrease in the expiratory reserve volume
- (C) It increases in patients with a history of heavy smoking
- (D) It increases with pulmonary contusions
- (E) It is smaller (ml/kg) in children than in adults
Mismatching of ventilation to perfusion in the lung is greatest in which of the following situations?
- (A) Awake patient, spontaneous ventilation, lateral decubitus position
- (B) Anesthetized patient, controlled ventilation, supine position
- (C) Anesthetized patient, controlled ventilation, lateral decubitus position
- (D) Anesthetized patient, controlled ventilation, sitting position
- (E) Anesthetized patient, spontaneous ventilation, prone position
A 157 cm (5 ft 2 in), 180-kg, 40-year-old woman has a PaO2 of 65 mmHg, a PaCO2 of 38 mmHg, and a pH of 7.43 while breathing room air preoperatively. The most likely cause of these values is
- (A) decreased hypoxic ventilatory drive
- (B) higher than normal oxygen extraction from blood
- (C) lower than normal cardiac output
- (D) lower than normal functional residual capacity
- (E) polycythemia
A 35-kg child requires mechanical ventilation with pure oxygen at a tidal volume of 350 ml and a rate of 20/min during a severe asthma attack. The most likely cause of severe hypotension after initiating mechanical ventilation is
- (A) hypoxic circulatory depression
- (B) inadequate expiratory time
- (C) increased pulmonary vascular resistance
- (D) respiratory alkalosis
- (E) tension pneumothorax
A healthy, spontaneously breathing, supine, anesthetized patient has an arterial to end-tidal carbon dioxide tension difference of 3 mmHg. Following institution of mechanical ventilation the value increases to 12 mmHg. The most likely cause of this change is
- (A) cephalad displacement of the diaphragm
- (B) decreased production of carbon dioxide
- (C) increased cardiac output
- (D) increased shunting of blood through dependent lung zones
- (E) increased ventilation of nondependent lung zones
Systemic hypothermia to 30°C is accompanied by
- (A) a shift to the right of the oxyhemoglobin dissociation curve
- (B) a decrease in carbon dioxide dissolved in plasma
- (C) a decrease in the glomerular filtration rate
- (D) an increase in MAC of volatile inhalation agents
- (E) low-voltage, high-frequency EEG pattern
Compared with a patient who is breathing spontaneously, a patient in the supine position receiving controlled positive-pressure ventilation will most likely have which of the following findings?
- (A) Decreased pulmonary vascular resistance
- (B) Decreased ratio of dead space to tidal volume
- (C) Increased ventilation of nondependent alveoli
- (D) Increased perfusion of nondependent alveoli
- (E) Improved matching of ventilation to perfusion
A 95-kg, 65-year-old woman receives sevoflurane and pancuronium during a laparoscopic cholecystectomy. Three minutes after administration of neostigmine 5 mg and atropine 1.2 mg, the twitch height returns to normal. Spontaneous tidal volume is 500 ml when the endotracheal tube is removed. In the PACU she reports dyspnea and appears distressed. Which of the following is the most likely cause of the respiratory distress?
- (A) Atelectasis
- (B) Cholinergic crisis
- (C) Pain
- (D) Residual enflurane
- (E) Residual muscle paralysis
A patient has decreased lung compliance and hypoxemia after a 30-minute episode of laryngospasm following extubation. The most likely cause is
- (A) allergic reaction to the anesthetic
- (B) altered alveolar-capillary membrane permeability
- (C) anesthetic-induced lymphatic dysfunction
- (D) increased pulmonary capillary pressure
- (E) negative pulmonary interstitial hydrostatic pressure
A 30-year-old man who is undergoing laparotomy and resection of a large kidney tumor has a decrease in SpO2 from 100% to 92% and an increase in peak airway pressure from 20 to 35 cm H2O. Plateau pressure is unchanged at 18 cm H2O. Which of the following is the most likely cause?
- (A) Abdominal packing
- (B) Inadequate anesthesia
- (C) Inadequate muscle relaxation
- (D) Obstruction of the endotracheal tube
- (E) Pneumothorax
Carbon dioxide retention first occurs when the ratio of forced expiratory volume in 1 second to vital capacity (FEV1/VC) decreases below
- (A) 15%
- (B) 35%
- (C) 50%
- (D) 65%
- (E) 75%
For any given FiO2 and PaCO2, the PaO2 is lower in a healthy paralyzed patient anesthetized with isoflurane than in the same patient unanesthetized and breathing spontaneously. The primary cause of this difference is
- (A) controlled ventilation
- (B) increased airway resistance
- (C) inhibition of hypoxic pulmonary vasoconstriction
- (D) intraoperative hypothermia
- (E) preferential ventilation of nondependent lung
Which of the lines shown in the graph illustrates the relationship of hematocrit and oxygen transport?
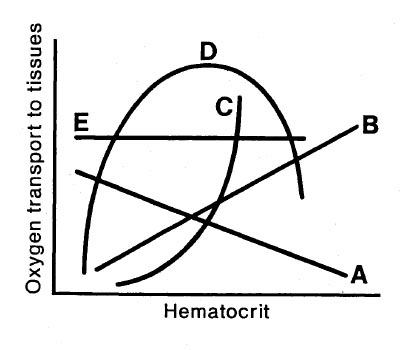
- (A) Line A
- (B) Line B
- (C) Line C
- (D) Line D
- (E) Line E
A 55-year-old man is undergoing craniotomy in the sitting position. Mean arterial pressure is 75 mmHg; arterial blood gas values are PaCO2 41 mmHg and pH 7.37. End-tidal CO2 is 7 mmHg. Which of the following is the most likely cause of the increased PaCO2 to PetCO2 gradient?
- (A) Decreased cardiac output
- (B) Endobronchial intubation
- (C) Hyperinflation of the lungs
- (D) Partial disconnect of the capnograph sample tubing
- (E) Venous air embolism
A 70-kg 24-year-old man with bilateral pneumonia whose lungs are being mechanically ventilated has the following measured parameters: tidal volume 750 ml; FiO2 0.7; rate 12/min; positive end-expiratory pressure 10 cmH2O; PaO2 75 mmHg; PaCO2 55 mmHg; pH 7.30. Which of the following alterations should be made in the ventilatory settings?
- (A) Decreasing positive end-expiratory pressure
- (B) Decreasing respiratory rate
- (C) Increasing fresh gas flow rate
- (D) Increasing FiO2
- (E) Increasing tidal volume
During a cardiac arrest with effective chest compression and positive-pressure ventilation, 50 mEq of sodium bicarbonate is administered. Which of the following is the most likely result?
- (A) Decreased mixed venous pH
- (B) Decreased SpO2
- (C) Increased PetCO2
- (D) Increased plasma lactate concentration
- (E) Increased serum potassium concentration
Which of the following findings is most likely in an 85-kg 30-year-old man who is breathing spontaneously through 6-mm endotracheal tube?
- (A) Decreased PetCO2
- (B) Decreased SpO2
- (C) Increased minute ventilation
- (D) Increased respiratory rate
- (E) Increased tidal volume
Each of the following findings is characteristic of restrictive lung disease EXCEPT
- (A) decreased elasticity of the lungs
- (B) decreased FEV1/FVC ratio
- (C) decreased inspiratory reserve volume
- (D) increased work of breathing
- (E) normal anatomic dead space
Alveolar dead space is decreased by
- (A) halothane anesthesia
- (B) positive end-expiratory pressure
- (C) deliberate hypotension
- (D) atropine premedication
- (E) decreased tidal volume
Which of the following factors causes a decrease in mixed venous oxygen saturation?
- (A) Arteriovenous fistula
- (B) Decreased hemoglobin concentration
- (C) Decreased oxygen consumption
- (D) Increased cardiac output
- (E) Nitroprusside toxicity
In a spontaneously breathing patient, each of the following increases the work of breathing EXCEPT
- (A) an increase in respiratory rate by 10/min
- (B) a decrease in lung-thorax compliance by 10 cmH2O
- (C) an increase in carbon dioxide production by 1 ml/kg/min
- (D) a decrease in PaO2 from 80 to 65 mmHg
- (E) a 0.1 increase in the ratio of dead space to tidal volume
Alveolar stability at varying lung volumes is maintained by
- (A) constant surface tension
- (B) increased surface tension at low lung volume
- (C) decreased surface tension at high lung volume
- (D) decreased surface tension at low lung volume
- (E) none of the above