10 Random Questions
A 70-kg, 50-year-old man is scheduled for muscle flap closure of a decubitus ulcer over the sacrum. He has been quadriplegic at the level of C6-7 for six years. Which of the following is most likely to result from subarachnoid anesthesia with tetracaine 10 mg for this procedure?
- (A) Atrioventricular block
- (B) Decreased risk for autonomic dysreflexia
- (C) Impaired expiratory muscle function
- (D) Impaired inspiratory muscle function
- (E) Inadequate block of spastic movements
Which of the following drugs used to produce or reverse muscle relaxation has the greatest prolongation of action in a patient with end-stage renal disease?
- (A) Atracurium
- (B) Neostigmine
- (C) Pancuronium
- (D) Succinylcholine
- (E) Vecuronium
The low fetal/maternal plasma ratio of bupivacaine compared with lidocaine is due to
- (A) fetal tissue binding
- (B) fetal plasma protein binding
- (C) maternal plasma protein binding
- (D) ionization in maternal blood
- (E) ionization in fetal blood
A normal adult is receiving general anesthesia via a standard circle system and controlled ventilation. Mass spectrometer data are shown. Which event is most compatible with these data?
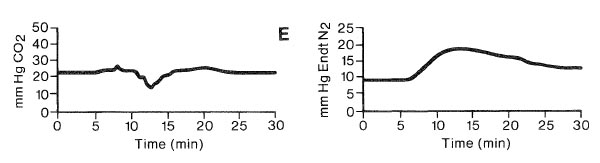
- (A) Endobronchial intubation
- (B) Hemorrhagic shock
- (C) Incompetent expiratory valve
- (D) Substantial decrease in fresh gas flow
- (E) Venous air embolism
During induction of anesthesia in a 70-year-old man with aortic stenosis, the blood pressure decreases from 140/ 80 to 70/45 mmHg as the cardiac rhythm changes from normal sinus at 70 bpm to junctional at 120 bpm. The most appropriate initial therapy would be
- (A) cardioversion
- (B) esmolol
- (C) fluid bolus
- (D) phenylephrine
- (E) verapamil
A 65-year-old patient with hypertrophic cardiomyopathy has chest pain prior to induction of anesthesia. Pulse is 80 bpm and blood pressure is 130/80 mmHg. The ECG (V5) shows sinus rhythm and new ST-segment depression. The most appropriate management is administration of
- (A) furosemide
- (B) metoprolol
- (C) morphine
- (D) nifedipine
- (E) nitroglycerin
Which of the lines shown in the graph illustrates the relationship of hematocrit and oxygen transport?
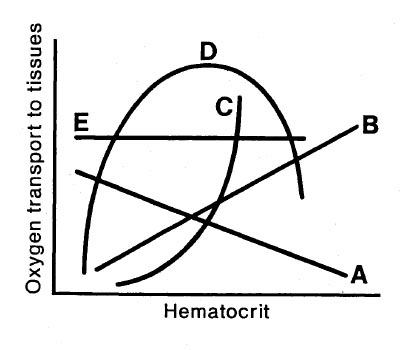
- (A) Line A
- (B) Line B
- (C) Line C
- (D) Line D
- (E) Line E
Which of the following findings differentiates the pickwickian syndrome from morbid obesity?
- (A) Carbon dioxide retention
- (B) Upper airway obstruction
- (C) Decreased forced expiratory volume
- (D) Increased shunt fraction
- (E) Increased functional residual capacity
In calculating the fluid requirements for a newborn undergoing repair of an omphalocele, the third-space loss should be replaced by
- (A) 0.9% saline solution
- (B) 2.5% dextrose in 0.45% saline solution
- (C) 5% dextrose in lactated Ringer's solution
- (D) 5% dextrose in water
- (E) 5% dextrose in 0.25% saline solution
The EEG of a patient undergoing anesthesia with high-dose fentanyl would most likely show
- (A) the same pattern seen with enflurane 0.5 MAC
- (B) cessation of low-frequency activity
- (C) accentuation of high-frequency activity
- (D) uniform depression of all frequencies
- (E) low-frequency, high-amplitude activity